Healthcare call centers operate under unusual pressure. They must manage high call volumes, protect sensitive information, comply with regulatory requirements, and maintain service quality; often within tight staffing constraints. Traditional call center optimization tactics, such as aggressively reducing handle time, rarely translate cleanly into better patient outcomes.
This guide outlines practical, defensible healthcare call center best practices grounded in routing logic, call center metrics, quality assurance, compliance controls, agent training, and technology integration. The focus is operational clarity: how to structure systems and oversight so patient communication is consistent, measurable, and aligned with clinical priorities.
Designing call routing around clinical urgency
Most call centers route based on agent skill groups: billing, support, scheduling, sales. That model works in commercial environments. In healthcare, it often creates risk.
A symptom-related call routed to a general queue may sit behind appointment confirmations. An urgent clinical concern may be transferred multiple times before reaching someone qualified to triage it. Each transfer increases frustration and, more importantly, delay.
Healthcare routing should prioritize clinical urgency first, department second.
Implement intent-based call routing for medical risk segmentation
Traditional skill-based routing assumes every call within a department carries equal weight. In healthcare, that assumption fails. A prescription refill and chest pain shouldn’t enter the same queue simply because both relate to “primary care.”
A more appropriate structure segments calls by intent and urgency at the earliest possible stage.
A practical framework looks like this:
- Administrative (address updates, insurance questions, appointment times)
- Prescription-related (refills, pharmacy coordination)
- Symptom-related (non-urgent) (new concerns, follow-up questions)
- Urgent clinical (severe symptoms, post-procedure complications)
The goal is to direct the call into the correct risk pathway quickly and consistently.
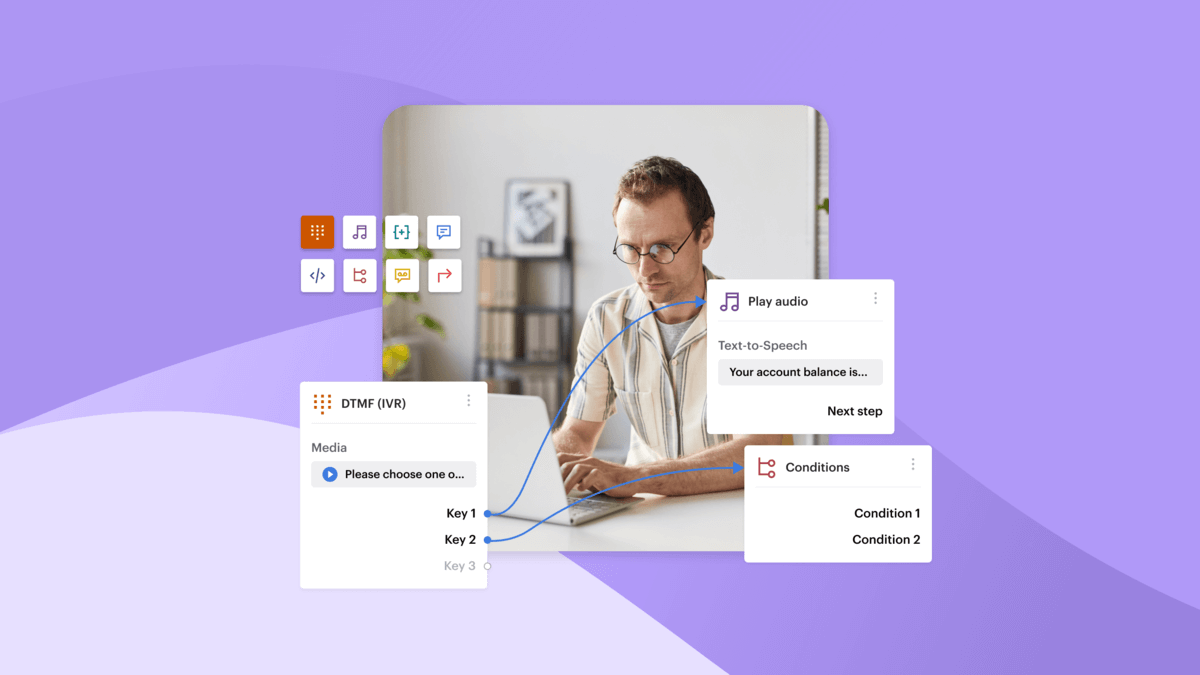
Using IVR pre-qualification logic
An IVR can perform structured pre-qualification using:
- DTMF input (“Press 1 for appointments, 2 for prescriptions, 3 for new or worsening symptoms”)
- Basic predefined speech input matching for configured intent phrases
- Fallback logic for unclear responses
This is rule-based routing, not AI interpretation. The system follows predefined logic trees.
KPIs that validate routing performance
Routing logic should be measured, not assumed to work.
Key metrics include:
- Transfer rate – High transfer rates often signal poor initial segmentation.
- Misroute percentage – Percentage of calls reassigned to a different queue.
- Time-to-clinical-response – Time from call entry to qualified clinical contact.
- Abandonment rate within symptom queues – Indicates whether urgent calls are waiting too long.
Reducing average handle time isn’t the primary objective in healthcare routing. Reducing delay for high-risk calls is.
Well-designed routing doesn’t eliminate operational pressure. It structures it. When urgency is embedded into the queue logic itself, the contact center becomes more predictable, measurable, and aligned with patient safety priorities.
Align call center metrics with patient outcomes, not just AHT
In most contact centers, performance discussions begin with average handle time (AHT). In healthcare, that starting point can be misleading.
Efficiency matters. But patient safety, clarity, and regulatory discipline matter more. The right metric framework reflects that balance.
Rethink core call center metrics in healthcare
Healthcare leaders still need standard operational visibility. Core metrics include:
Operational metrics
These indicators reveal capacity, staffing alignment, and workflow friction. They are necessary. But, they’re not sufficient.
Healthcare environments require additional measures that reflect clinical and regulatory realities.
Healthcare-specific metrics
- Time-to-triage – Time from call entry to contact with a clinically qualified agent.
- Escalation accuracy rate – Percentage of urgent calls correctly routed to clinical staff without reclassification.
- Repeat call rate for the same issue – Often signals incomplete resolution or unclear guidance.
- Compliance adherence score – Percentage of calls meeting identity verification and disclosure protocols.
These measures shift the focus from speed alone to structured, safe resolution.
The AHT trade-off
Reducing AHT can appear positive on dashboards. In healthcare, aggressively pushing for shorter calls may reduce clarification, increase patient confusion, or lead to repeat contacts.
Research from organizations such as McKinsey has consistently shown that clarity and confidence during service interactions are stronger predictors of satisfaction than raw speed. In healthcare, rushed conversations can also increase compliance exposure.
This doesn’t mean AHT is irrelevant. It means it must be interpreted alongside:
- Repeat call rate
- Escalation accuracy
- Compliance adherence
If handle time decreases while repeat calls rise, the system is not improving. It is deferring resolution.
Healthcare call center metrics should reflect the full patient journey, not just queue throughput.
Use conversation analytics for quality assurance and risk monitoring
Manual call sampling provides limited visibility. In healthcare environments, limited visibility creates risk.
Conversation analytics adds structured oversight after the call has taken place. It doesn’t guide agents in real time, but it helps supervisors review patterns, identify gaps, and prioritize coaching.
Voiso’s AI Speech Analytics provides post-call transcripts, keyword grouping, and call scoring. Supervisors can review call summaries and analyze interaction trends without listening to every recording. The system surfaces structured data from conversations; it doesn’t make autonomous compliance decisions.
Topic identification and sentiment tracking
Topic grouping allows teams to:
- Identify high-frequency complaint categories
- Track symptom-related call volumes
- Monitor escalation themes
Post-call sentiment indicators can help supervisors identify calls for review. These signals support investigation; they don’t replace human judgment.
Script adherence and compliance keyword monitoring
Healthcare calls often require structured identity verification and regulated language.
Keyword monitoring can allow supervisors to:
- Surface calls where verification phrases may be missing.
- Flag sensitive terms (e.g., account numbers, diagnosis references)
- Review calls where required disclosures may have been skipped
This supports compliance oversight but doesn’t guarantee regulatory adherence.
Practical QA use cases
- Missed identity verification: If required verification phrases are absent from transcripts, those calls can be flagged for review and coaching.
- Emotional distress detection: Calls containing repeated high-stress keywords or negative sentiment patterns can be prioritized for supervisory follow-up.
- Protected health information (PHI) disclosure monitoring: Keyword filters can surface calls where sensitive data was discussed, enabling audit review and process correction.
In each case, analytics provides structured visibility. Human supervisors interpret the context and determine corrective action.
Build compliance into everyday workflows
In healthcare contact centers, compliance can’t exist as a policy document alone. It has to be embedded into how calls are routed, handled, logged, and reviewed.
When compliance controls are separated from daily operations, gaps appear. The goal is to create repeatable execution.
Embed HIPAA and data protection controls into call flows
Handling protected health information (PHI) begins with structured process design.
At the operational level, this typically includes:
- Mandatory identity verification before disclosing patient data
- Clear escalation paths when verification cannot be completed
- Defined language protocols for discussing diagnoses, billing, or insurance details
These steps should be embedded into the call workflow itself.
Mandatory verification before disclosure
Before sharing medical or billing information, agents should complete predefined verification steps, such as confirming date of birth or other approved identifiers.
Verification requirements can be reinforced through:
- Script guidelines in training materials
- QA keyword monitoring (reviewed post-call)
- Call flow checkpoints in IVR before routing to sensitive queues
The objective is consistency. Every call involving PHI should follow the same verification structure.
Role-based access controls
Not every agent should have access to the same level of patient information.
Operationally, this means:
- Segmenting queues by function (e.g., scheduling vs. billing vs. clinical triage)
- Restricting data visibility based on role
- Logging activity for audit review
A contact center platform can support structured access management and call logging, but compliance oversight remains a management responsibility. Technology enables control; it doesn’t replace governance.
Automate compliance audits using QA technology
Traditional quality assurance relies on manual sampling. Supervisors review a small percentage of calls and score them against internal checklists.
This approach has limits:
- It covers only a fraction of total volume
- It depends heavily on reviewer consistency
- It may miss isolated but high-risk incidents
Speech analytics expands visibility by structuring data from every recorded call. It doesn’t replace human review, but it helps teams prioritize where to focus.
Manual sampling vs. structured full-call visibility
- Manual sampling offers depth but limited breadth.
- Analytics-assisted review offers breadth and pattern detection, followed by targeted human investigation.
This hybrid model allows supervisors to concentrate on calls that show potential compliance gaps rather than reviewing randomly selected interactions.
Conversation scoring and review efficiency
Post-call scoring provides a structured signal that can reduce the time needed to identify outlier conversations. Low-scoring calls or those containing predefined sensitive keywords can be reviewed first.
This doesn’t automate compliance decisions. It shortens the path to meaningful review.
Connecting QA findings to performance management
Compliance monitoring is most effective when findings feed directly into coaching.
For example:
- Repeated missed verification steps → targeted retraining
- Frequent disclosure errors → workflow adjustments
- Consistent confusion around specific policies → script clarification
Compliance shouldn’t function as a punitive exercise, but as a feedback loop.
When compliance controls are embedded into routing, recording management, transcript review, and coaching cycles, risk management becomes operational rather than reactive.
Strengthen agent training through data-backed coaching
Healthcare call center work is cognitively demanding. Agents manage administrative requests, emotional conversations, and regulated disclosures, often within the same shift. Training cannot rely on theory alone. It needs to reflect what actually happens on live calls.
Data-backed coaching uses real interaction evidence to improve performance in a structured, measurable way.
Use real interaction data for targeted skill development
Generic feedback such as “be more empathetic” or “reduce handle time” rarely changes behavior. Coaching becomes more effective when it’s anchored to specific calls.
Call recordings and transcripts provide that anchor.
Conversation scoring can also provide a structured assessment based on language patterns and interaction dynamics.
Turning QA results into structured improvement plans
Quality assurance findings should translate into defined actions, not general reminders.
For example:
- Repeated missed verification steps → focused compliance refresher
- Overly short calls in complex cases → coaching on clarification techniques
- High repeat call rate linked to specific agents → resolution quality review
A structured improvement plan typically includes:
- Call examples reviewed together
- Clear behavioral expectations
- Follow-up evaluation within a defined timeframe
The goal is consistency. Data makes feedback specific. Specific feedback makes improvement measurable.
Reduce agent burnout with smart workload management
Healthcare call centers expose agents to high emotional intensity. Symptom escalation, billing disputes, and distressed callers accumulate cognitive strain over time.
Burnout affects:
- Communication clarity
- Patience
- Compliance adherence
- Retention
Managing workload is therefore a performance issue, not just an HR concern.
Blended channel handling
Not all interactions require the same emotional bandwidth.
When configured carefully, blending channels such as voice and messaging can distribute cognitive load. Lower-intensity administrative requests may be handled via messaging queues, while symptom-related calls remain prioritized for voice.
This requires thoughtful routing and queue configuration. It is not automatic. Supervisors must monitor volume and adjust capacity accordingly.
Supervisor visibility and intervention
Operational dashboards and live monitoring tools allow supervisors to observe queue conditions and intervene when necessary. Supervisors can listen to calls, provide guidance where appropriate, and redistribute workload if certain queues become overloaded.
These tools support oversight. They don’t automate decision-making.
Linking burnout reduction to patient outcomes
Agent fatigue doesn’t remain internal. It appears in tone, clarity, and patience. Over time, this affects:
- Patient satisfaction scores
- Repeat call rates
- Escalation errors
Healthcare service research consistently shows that perceived empathy and clarity strongly influence patient trust and retention. Protecting agent wellbeing therefore supports both compliance stability and long-term patient loyalty.
Structured coaching and controlled workload are connected. When supervisors use interaction data to guide development—and monitor operational pressure in real time—the contact center becomes more stable, predictable, and resilient.
Integrate technology to eliminate information silos
In many healthcare environments, patient communication tools and patient data systems operate separately. Agents toggle between the phone system, the CRM, scheduling software, and sometimes an EHR interface. Every switch increases handling time and raises the risk of incomplete documentation.
Unify CRM and call center systems for complete patient context
When call systems and CRM platforms are disconnected, agents work with partial visibility. They may not see prior interactions, unresolved issues, or recent updates before answering the call. This affects both resolution quality and documentation accuracy.
A unified workflow typically includes:
- Screen pop when a call matches an existing contact record
- Automatic call logging within the CRM
- Logged call activity in the CRM to maintain interaction history
Voiso supports CRM integrations, including Zoho, Salesforce, and Freshdesk. These integrations can enable agents to initiate calls from within the CRM interface (where supported), view matched contact information when a call arrives, and automatically log call activity after the interaction.
This doesn’t mean Voiso replaces the CRM or stores patient records independently. The CRM remains the system of record. Voiso supports call execution and activity logging within that workflow.
Operational impact
When call logging is automated and patient context is visible at call start:
- First call resolution (FCR) often improves because agents do not need to re-collect known information.
- Repeat calls decrease when documentation is consistent.
- Audit readiness improves because interaction history is centralized.
Integration doesn’t guarantee better outcomes. It creates the conditions for more consistent documentation and faster context retrieval.
Expand beyond voice with omnichannel patient communication
Voice remains central in healthcare. However, not every interaction requires a live call.
Patients increasingly expect confirmation messages, follow-up details, and non-urgent updates through digital channels.
SMS appointment reminders
SMS remains one of the most direct communication methods. Industry data consistently shows SMS open rates near 98%, with most messages read within minutes of receipt. For appointment reminders, this can reduce no-shows and lower inbound confirmation calls.
Voiso supports SMS capabilities that can let agents send follow-up messages during or after calls. This supports continuity but doesn’t replace scheduling systems.
Omnichannel engagement and cross-channel handover
Omnichannel workspaces can support managing voice and configured messaging channels within a shared interface. Interaction history can be viewed within supported channels when properly configured.
This doesn’t mean channels are automatically synchronized across external systems. Configuration and operational discipline remain necessary.
When voice deflection reduces congestion
Deflecting appropriate low-risk inquiries, such as appointment confirmations or document requests, from voice to messaging can help preserve capacity in symptom-related or urgent queues.
This requires:
- Clear IVR prompts
- Defined deflection rules
- Monitoring to ensure urgent calls are not misdirected
Deflection should never apply to high-risk symptom calls. It should support queue stabilization, not reduce access.
SLA tracking across channels
As communication expands beyond voice, service level agreements (SLAs) must extend across channels. Supervisors need visibility into:
- Response times for messaging queues
- Abandonment or timeout patterns
- Channel-specific volume trends
Operational dashboards can support this oversight. Consistent monitoring ensures that expanding channels doesn’t create new blind spots.
Solve the most common healthcare call center bottlenecks
Healthcare call centers rarely fail because of a single issue. Most operational strain comes from predictable bottlenecks that compound over time: misrouted calls, incomplete documentation, uneven workload, and limited QA visibility.
This means it’s key to address root causes directly rather than treating surface symptoms.
Below is a structured breakdown of common challenges, what typically causes them, and practical corrective actions.
| Operational challenge | Root cause | High-impact solution |
| High abandonment rate | Poor routing logic | Intent-based IVR + callback configuration |
| Compliance violations | Manual QA sampling | Post-call keyword monitoring + targeted review |
| Long handle times | No CRM integration | Screen pop + automatic call logging |
| Agent burnout | Emotional overload | Live supervisor visibility + structured coaching |
| Repeated patient calls | Poor documentation | CRM integration + standardized call summaries |
How to apply these solutions
High abandonment rate: If abandonment is concentrated in symptom-related queues, review routing segmentation first. Introduce clearer IVR pathways and configure callback options for lower-risk inquiries to protect urgent queues.
Compliance violations: When QA relies only on random sampling, visibility is limited. Introduce structured transcript review using keyword monitoring to surface calls requiring human audit. This expands oversight without increasing manual review volume indiscriminately.
Long handle times: If agents toggle between multiple systems during each call, integration should be prioritized before coaching speed. Screen pop and automatic call logging reduce administrative overhead and allow agents to focus on resolution rather than documentation mechanics.
Agent burnout: When emotional intensity remains consistently high, supervisors need real-time operational visibility. Monitoring queue pressure and redistributing workload early prevents sustained overload. Coaching should address both technical accuracy and emotional resilience.
Repeated patient calls: High repeat rates often indicate unclear documentation or incomplete resolution. Standardized call summaries and consistent CRM logging create continuity across interactions and reduce rework.
Each of these bottlenecks is measurable. Each has an operational fix. The impact comes from disciplined implementation rather than isolated feature adoption.
The future of healthcare call centers: Predictive, preventive, and personalized
Done right, the future of healthcare call centers is about smarter use of operational data.
Teams are using historical call patterns to improve staffing decisions and reduce congestion during predictable peak periods. Post-call analytics, including call score indicators and keyword trends, help supervisors identify escalation patterns and refine routing logic over time.
AI-assisted call summaries can support more consistent documentation review.
For outbound appointment confirmation campaigns, AI Answering Machine Detection (AMD) helps limit time spent on voicemail by identifying whether a live person answers before connecting the call to an agent .
The direction is practical: better forecasting, clearer oversight, and more structured communication; while keeping clinical judgment and compliance control firmly in human hands.
FAQs
What are the most important healthcare call center metrics?
Healthcare call center best practices go beyond average handle time (AHT). While operational metrics like AHT, abandonment rate, queue time, and first call resolution (FCR) remain important, healthcare teams should also track time-to-triage, escalation accuracy, repeat call rate, and compliance adherence. These additional metrics reflect patient safety, documentation quality, and regulatory discipline, not just speed. A balanced scorecard prevents efficiency targets from undermining clinical responsiveness.
How can healthcare call centers improve compliance monitoring?
Compliance monitoring improves when oversight is embedded into daily workflows. This includes structured identity verification processes, role-based data access, and consistent call logging. Post-call transcript review and keyword monitoring can help supervisors identify missed disclosures or verification steps. These tools support broader visibility, but they don’t replace human audit review. Effective compliance monitoring combines structured process design with targeted quality assurance.
What technology is essential for modern healthcare contact centers?
Modern healthcare contact centers typically require structured routing logic, secure call recording, CRM integration for context visibility, and operational reporting. Integration between the call platform and CRM system supports screen pop and automatic call logging . Rule-based IVR configuration helps segment calls by urgency . These capabilities provide operational structure; clinical systems of record remain separate.
How does AI improve patient communication in call centers?
AI in healthcare contact centers is typically used for post-call analysis rather than live intervention. Speech analytics can generate transcripts, identify recurring topics, and provide structured conversation scoring. These insights help supervisors detect trends, prioritize coaching, and monitor compliance. AI does not replace clinical judgment or make autonomous decisions. It supports oversight and pattern recognition after the interaction.
How do you reduce abandonment rates in healthcare call centers?
Reducing abandonment begins with better routing and queue prioritization. Intent-based IVR paths help separate administrative calls from symptom-related calls early in the flow. Callback options for non-urgent inquiries can help preserve capacity in higher-risk queues. Historical call data can inform staffing adjustments during predictable peak periods. Abandonment is usually a systems issue, not just a staffing issue.